Diabetic foot risk stratification and triage
Select the crosses on the image below for more detail
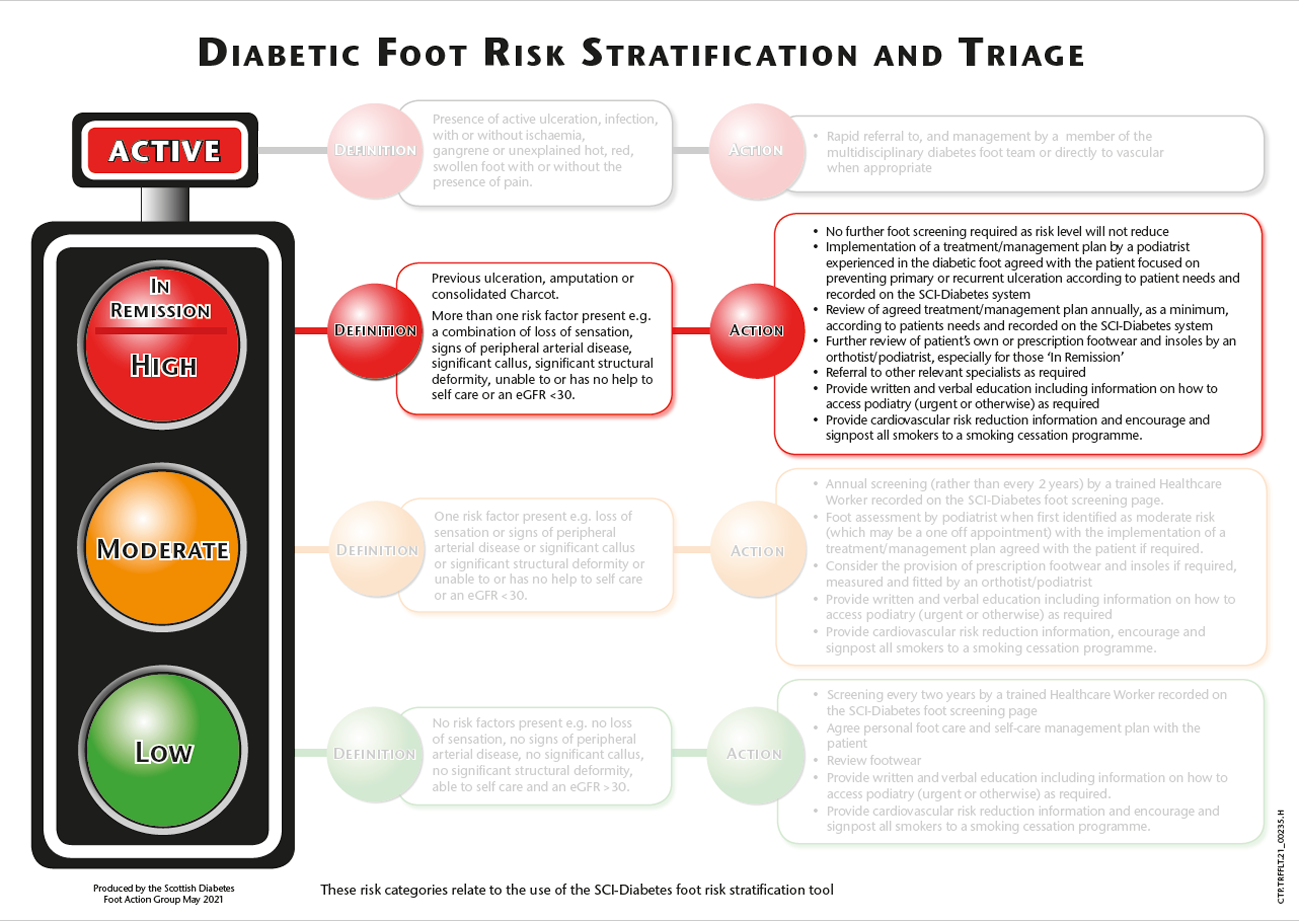
These risk categories relate to the use of the SCI-Diabetes foot risk stratification tool
Select the crosses on the image below for more detail
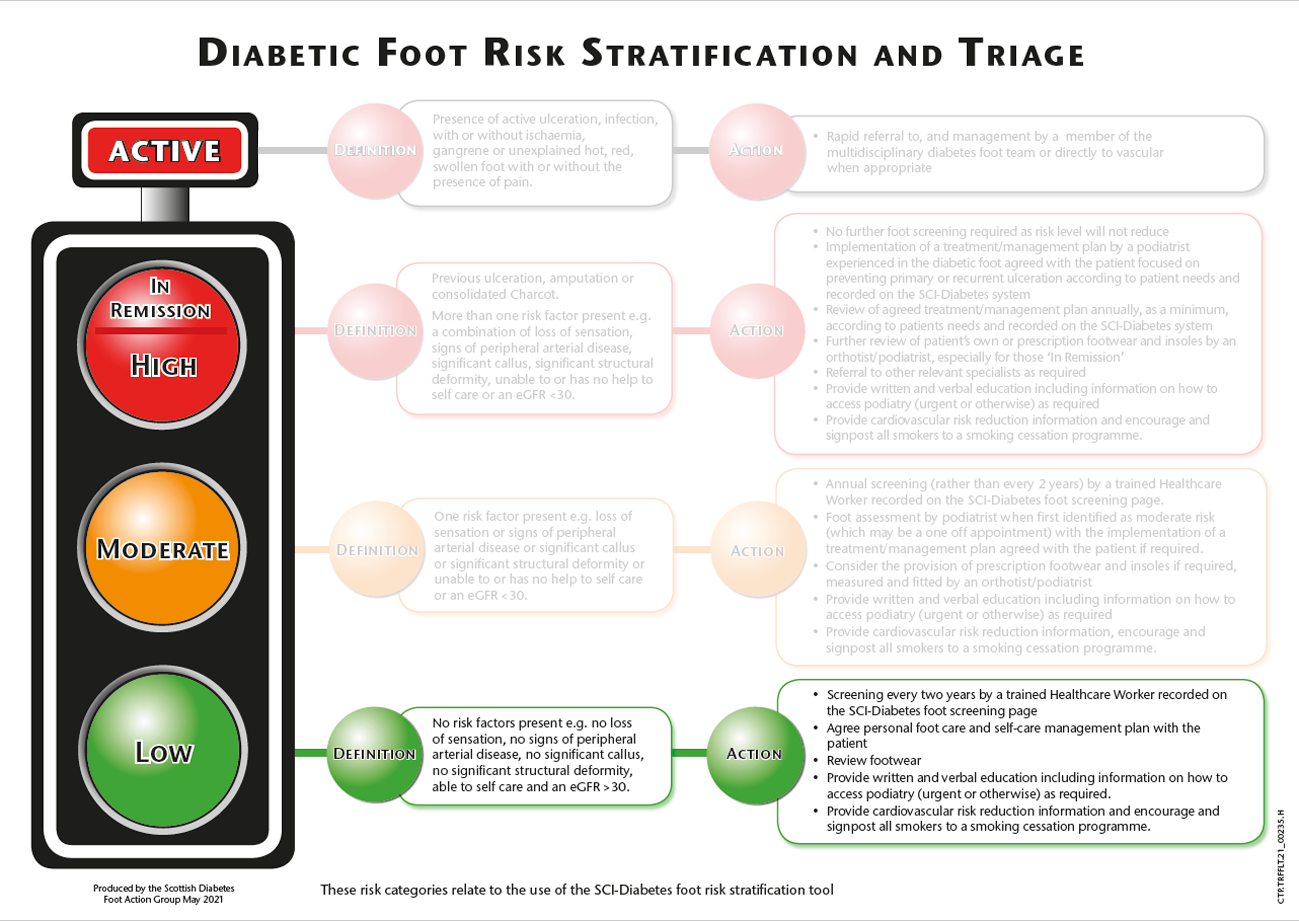
These risk categories relate to the use of the SCI-Diabetes foot risk stratification tool

These risk categories relate to the use of the SCI-Diabetes foot risk stratification tool
These risk categories relate to the use of the SCI-Diabetes foot risk stratification tool

These risk categories relate to the use of the SCI-Diabetes foot risk stratification tool
These risk categories relate to the use of the SCI-Diabetes foot risk stratification tool
The process of foot screening must lead to the individual with diabetes being assigned a risk category, and informed of and understand what that risk category means to them as an individual living with diabetes. According to the assigned risk category this will result in the introduction of a treatment/management plan according to that risk level formulated in consultation with the individual with diabetes, tailored to suit their needs.
The validity of diabetic foot screening is optimized if the process is carried out and recorded in a standardised manner wherever the individual is seen. It is recommended as an area of good practice within the sign guideline that:
‘The result of a foot screening examination should be entered onto an online screening tool, such as the Scottish Care Information – Diabetes Collaboration system (SCI-DC), (now known as SCI – Diabetes), to provide automatic risk stratification and a recommended management plan, including patient information’.
Foot screening may be carried out by any health care professional/worker involved in the care of an individual with diabetes. Examples of these could include the following: podiatrist, podiatry technician, practice nurse, support worker, district nurse, General Practitioner or any other competent healthcare worker.
It is not important who undertakes the screening process as long as the individual carrying this out has the capability and training to do so and is aware of what action to take depending on the results and the individual with diabetes risk status. This capability can be gained by undertaking this training and the test at the end of this module.
The guideline simply states that:
‘All patients with diabetes should be screened to assess their risk of developing a foot ulcer’.
It also stated that:
‘There is no evidence to support the frequency of screening; however the SIGN guideline group considers that at least annual screening from the diagnosis of diabetes is appropriate’.
Following wide consultation with the Scottish Diabetes Foot Action Group it was decided to update our Traffic Light System (2016) and subsequently the way foot screening is delivered in Scotland to reflect recent evidence (Leese et al 2006), (Crawford et al 2020) and to ‘mirror’ some of the changes that have been introduced to the national Diabetes Retinal Screening (DRS) programme.
The purpose of diabetic foot screening is to carry out a quick, simple, and evidence based screening to determine at what risk an individual is of developing a diabetic foot ulcer, which may lead to an amputation. The individual should be made aware of their foot risk status and have an appropriate treatment/management plan agreed with the individual and implemented if/when required.
The Scottish Intercollegiate Guidelines Network (SIGN 116) is produced in Scotland to guide clinicians on the most up to date, and evidence based practice. This guideline will mainly be of interest to all healthcare professionals/workers involved in the care of individuals with diabetes. The target users are, however, much broader than this, and include individuals living with diabetes, their carers and those who interact with individuals with diabetes outside of the NHS. It will also be of interest to those planning the delivery of services in NHS Scotland and beyond.
The guideline states that:
‘Diabetic foot screening is effective in identifying the level of risk of developing foot ulceration in patients with diabetes’.
It also focuses on keeping the screening process simple and ensuring that all the main risk factors are screened for:
‘Simple tests such as the use of 10g monofilament, palpation of pulses, neuropathy disability score, presence of significant structural abnormality and previous ulceration, when routinely used during screening are effective at predicting ulceration’.
The screening process for PAD is simple and consists of checking, via palpation, for the two pulses in each foot. If either of these pulses are present during the screening process then the circulation to the foot is perceived to be adequate. These pulses are the Dorsalis Pedis (DP) and the Posterior Tibial (PT). The individual should be asked if they have any signs of intermittent claudication (cramping in the calf muscle after walking a certain distance) and also be given advice regarding lifestyle changes, most importantly stopping smoking.
If during the screening process neither of the pulses can be palpated or the individual presents with any of the aforementioned problems they may need to be referred for a more in depth assessment of their PAD, leading in some cases to the implementation of an Education / Management plan to try and improve the situation or referral to vascular services for surgical intervention where appropriate.